By Barry Cole, MD
In May 1980, six weeks before I started my residency training, the American Psychiatric Association released the Diagnostic and Statistical Manual of Mental Disorders, 3rd edition (DSM-III). At once, the philosophy of psychiatry shifted from being brainless to being mindless.
The specialty of psychiatry moved from psychological to physiological, to see itself as a sub-discipline of neuroscience. What I experienced during my psychiatry residency turned out not to be what I planned when I decided to become a psychiatrist. My residency director informed me that in the “DSM-3 world” I made diagnoses based upon objective inclusion criteria, no longer based on fuzzy exclusion criteria, impressions, intuition, and most definitely not by “feeling a glass wall between us.”

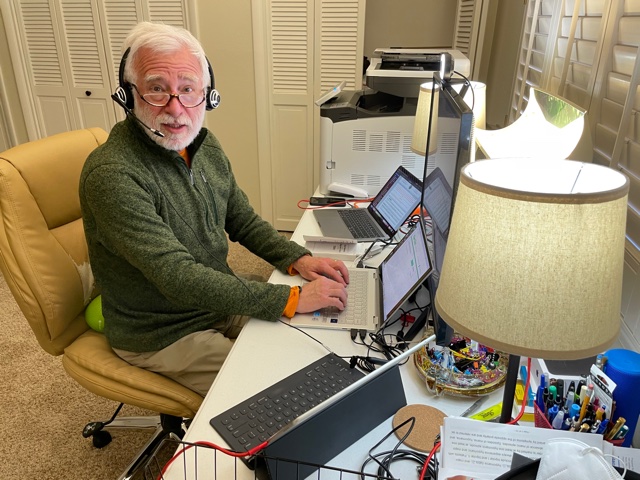
Dr. Barry Cole uses tele-psychiatry during the COVID-19 epidemic to stay in touch with patients.
I was expected to prescribe medication, order laboratory and imaging studies, consult with neurologists about electrophysiological examinations, refer my patients to other providers for therapy services (not provide them personally), and see myself as a physician specializing in mental health.
During the last 40 years, what I prescribed evolved from 3 monoamine oxidase inhibitors, many tricyclic antidepressants, several traditional antipsychotics and lithium, to selective neurotransmitter-specific antidepressants, second-generation antipsychotics, many different mood stabilizers, and using a few benzodiazepines and z-drugs as infrequently as possible. The role for rational polypharmacy came to influence my medication decision-making, so the question to be answered wasn’t which medication was best, but what combination of medications, each working by different mechanisms of action, gave the best outcome with the fewest side effects.
I learned to be incremental in prescribing, starting low and moving upward slowly, and seeing symptoms respond over weeks or months.
Understanding what people are experiencing
Some of what I learned during my residency and fellowship training was by trial and error. I found it unsatisfying to not understand what people were experiencing, which medication was most needed (as if there was only one correct option), what had I missed along the way that might have significant potential for harm, and if people with their disorders were really that different as we tried to define them ever more precisely with each generation of the DSM. My training was done on the job, attending lectures and demonstrations, reading books and journals, providing day-to-day care, and then struggling to make sense out of nonsense, chaos, and stay within the lines created by regulatory entities (e.g., medical board, pharmacy board, Drug Enforcement Administration, Food and Drug Administration, Center for Disease Control).
Over 40 years, I have at times never written opioid prescriptions; later, I wrote opioid prescriptions liberally; and now I fear opioids and rarely prescribe them to any of my patients. I have learned my craft by doing private practice, working for state and private health-care authorities, providing services for several not-for-profit organizations, and continuing my education into areas that I never knew existed until I found myself taking a class at UCLA (best class was on hypnosis), UNLV (best class was Political Economy during my master’s program in Public Administration) and attending as many conferences I could, deliberately picking sessions to attend based on what I didn’t already know.
At times I cared for a few inpatients, managed hundreds of outpatients, set and managed expectations for thousands of organization members. The differences between individual care and organizational needs intrigued me. Were organizations just groups of individuals with needs, or was there more to satisfying people belonging to a professional society, making their lives more predictable?
A self-evident truth
Over 40 years in Nevada, key decision-makers moved from feeling shame about our mental health system being marginal (saying “Thank God for New Mexico, Louisiana, Mississippi, and Alabama!”) to accepting being ranked last in the nation for eight consecutive years (due to our limited services and their access). I recall members of the Legislature knowing their role in “playing the game.” Certain members of the Legislature knew that to properly fund the state mental health system they had to ask me “So, if we find an extra million or two dollars do you have ideas or plans for how you’d use that money?” I knew to go to Carson City with a list of projects I wanted, and to be able to produce that list on cue. However, over the years the same truth was always self-evident: “when the state budget doesn’t balance, take it from mental health, they (assumed to be the sufferers and their family members) don’t vote, so won’t impact election outcomes for any office holder.”
Tele-psychiatry has allowed me to enter homes, see my patients in their own lives, and see them as part of their families and communities.
A new reality
Covid-19 brought us a new reality, that face-to-face care is not the only option, there are other effective ways to deliver service. Tele-psychiatry has brought access to care for people from their homes, over their cell phones, from the safety of their living rooms, bedrooms, offices, kitchens. It has showed me a world never fully known to me. Tele-psychiatry has allowed me to enter homes, see my patients in their own lives, and see them as part of their families and communities. Tele-psychiatry is different than face-to-face encounters, as many of the cues I get from watching people walk from the waiting room — being able to smell for the presence of alcohol, cannabis, or even cologne or perfume — I don’t get over the internet. Instead of seeing the “whole” person, I see a rectangular image of them, with clear horizontal and vertical boundaries.
My patients have the ability to hide things from me easily, keep them off camera, and my goal is to bring human connection to the video encounter. There are few training programs for exactly how to do tele-psychiatry, but through repeated interactions, I have trained myself to maintain more eye contact, to use slightly exaggerated gestures that are easier to understand when televised, and do things to make my connection be effective, genuine and thoughtful.
Have the patients changed too?
Have patients changed over 40 years? I often think I now see more people with underlying personality disorders, more with out-of-control substance-use disorders and struggling with complex medical conditions manifesting as symptoms of mental disorders. I am not sure if patients have individually changed over the years, but serial DSMs have renamed disorders and encouraged me to be more specific about diagnosis.
Psychiatry has evolved and now requires a greater command of neuroscience, psychopharmacology, understanding drug-drug interactions and interferences, appreciation of metabolism and how medications I prescribe alter it, integrating genetics and gene penetrance into clinical decision making.
I practice tele-psychiatry with three computers running simultaneously and a 32-inch monitor so I can “see” my patients, view their medical records, and manage all of the information needed to be helpful. My greatest fear is forgetting or not observing something important, missing some objective finding because it is off screen, not running a drug-drug interaction check for every medication taken — not just the ones I prescribe — figuring out what motivates my patients to go for their necessary laboratory studies, and accepting how little I know yet how significant my decisions are. After 40 years, I accept that it’s often clearer for me to match the specific effects of medications to signs and symptoms I observe or to disorders they can improve according to their licensed indications, while addressing interferences by non-psychiatric medications and conditions, and carefully setting and then managing expectations.
What lies ahead
Near the end of my career, I am asked by some “What’s the future of psychiatry?” I don’t know, yet I see greater convergence between neuroscience and classical psychiatric skills. I suspect we will understand the expression of mental disorders through the lens of underlying neurobiology with some degree of humanism. Mental disorders will never be “cut and dry” like surgical conditions. My treatments will always require collaboration and a process where both the doctor and patient develop trust.
I am not sure if there’s going to be a significant increase in the pipeline producing psychiatrists, but if there isn’t, the national shortage will continue and worsen. That may lead to further development of alternative options: psychiatric nurse practitioners, prescribing authority for psychologists and pharmacists, and perhaps development of psychiatric physician assistants. We cannot continue to do the same over and over again, expecting the outcome to change. A famous saying told us what that defined.
So why did I enter psychiatry so long ago? When I rotated through the various specialties during medical school, the only one that was fun was psychiatry. Other specialties were interesting, cutting edge, interspersing stimulation with a bit of terror. But psychiatry was fun, and the people I met were truly interesting.
It has been an amazing 40 years, and I have been privileged to enjoy a front row seat to the incredible range and potential of the human mind. When I eventually retire, I will most miss my interactions with people.
Dr. Barry E. Cole is a psychiatrist in Reno, Nevada, and has been in practice for more than 40 years. You can listen to an interview with him by Joe Schoenmann on KNPR about coping with COVID-19 stress.




{kind=link}
{kind=link}
{kind=link}
{kind=link}